Amyotrophic lateral sclerosis (ALS) is a neurodegenerative disease that results in the progressive loss of motor neurons that control voluntary muscles. It is designated as a rare disease due to its low prevalence in the general population, which also fluctuates among different regional groups.
Epidemiological Studies of ALS
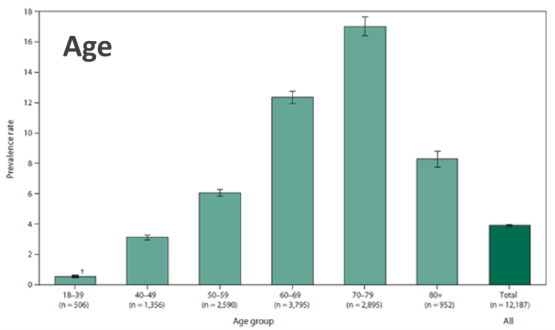
Epidemiological studies have found that the incidence of ALS is 1.9/105, the prevalence is 4.5/105, and the average age of onset is 55 years (Incidence: proportion of new patients per year; Prevalence: ratio of existing patients to total population).
(Source: Centers for Disease Control and Prevention)
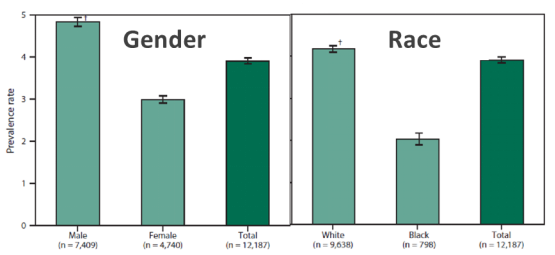
In addition, the data shows that the incidence rate in Europe and the United States is higher, at 2.6/105, and the prevalence rate is almost double, at 7-9/105. ALS is more common in men than women, and more common in whites, among whom Anglo-Saxons and Germanics have significantly higher rates than Latinos.
(Source: Centers for Disease Control and Prevention)
In contrast, the incidence is lower among asians, being as low as 0.8/105 in East Asia and 0.7/105 in South Asia. Because of this, Europe and the United States have invested heavily in the research of this disease, accounting for more than 80% of the world's research projects on ALS.
Motor Neuron Disease
ALS is a motor neuron disease (MND), which is a group of neurological disorders that selectively affect motor neurons with secondary damage to muscles. In a normal body, there is a motor nervous system that works in an orderly manner, as shown below:
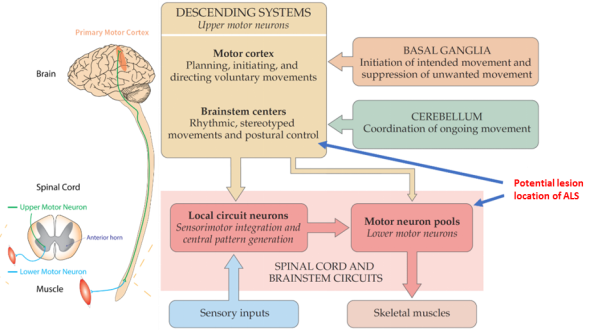
First, the motor cortex and brainstem in the brain transmit signals for active movement. The motor cortex is responsible for planning, initiating, and directing voluntary movements; the brainstem is responsible for rhythmic, stereotyped movements, such as breathing and postural control, which basically does not require the participation of active consciousness.
As supplementary areas of the brain, the basal ganglia is responsible for the initiation of intended movement and suppression of unwanted movement; the cerebellum is responsible for coordinating the functions of various departments during the whole process of movement and is in charge of coordinating ongoing movement.
Signals from the motor cortex and brainstem are transmitted to the spinal cord or motor neuron pools. Some information goes directly to the motor ganglia, and some is transmitted to the motor neuron pools through the spinal cord.
Then, the motor neurons in the motor neuron pools begin to order the muscles to work. At the same time, the spinal cord is responsible for sensorimotor integration and central pattern generation through local circuit neurons, handling simple problems and reporting complex problems to the motor cortex or brain stem for instructions.
It should be noted that two new terms are introduced here, Upper Motor Neuron (UMN) and Lower Motor Neuron (LMN). The former refers to the cortex without direct communication with the muscles, namely the neurons in the brainstem and spinal cord (excluding neurons in the supplementary area such as the cerebellum and basal ganglia); the latter refers to the neurons connected to the motor nerves.
The potential lesion location of ALS occurs in the chain of command transmission formed by these two types of neurons. The muscles are not diseased, but actually atrophy as nerve activity decreases.
Classification of ALS
According to the classification of the motor nervous system, ALS can be divided into two types: LMN-impaired and UMN-impaired.
The key to distinguishing the two is that the LMN-impaired type occurs directly in the neurons that communicate with the muscle from the beginning, so the symptoms are flaccid paralysis, hypomyotonia and hyporeflexia, convulsions and spasms, and a negative Babinski sign. The UMN-impaired type results in spastic paralysis, hypermyotonia and hyperreflexia, disuse-atrophy, and a positive Babinski sign.
Babinski sign:
The Babinski sign refers to a reflex elicited when the sole of the foot is stimulated with a blunt instrument. The reflex can take one of two forms. In healthy adults, the plantar reflex causes a downward response of the hallux (flexion). An upward response (extension) of the hallux is known as the Babinski response or positive Babinski sign, named after the neurologist Joseph Babinski. [2]
In addition, muscle atrophy of the LMN-impaired type occurs earlier and more rapidly than that of the UMN-impaired type, and the latter has a certain degree of muscle hyperfunction in the early stage.
The lesions of ALS are mainly located in motor neurons, but diagnosis is not easy because its symptoms are similar to those of many cerebellar and muscle atrophy-related diseases. In particular, UMN-impaired ALS is often confused with primary lateral sclerosis (PLS), which is also a UMN-impaired disease. LMN-impaired ALS and progressive muscular atrophy (PMA) are also indistinguishable.
Some countries simply classify PLS and PMA as ALS. Due to unclear classification, many epidemiological statistical results vary.
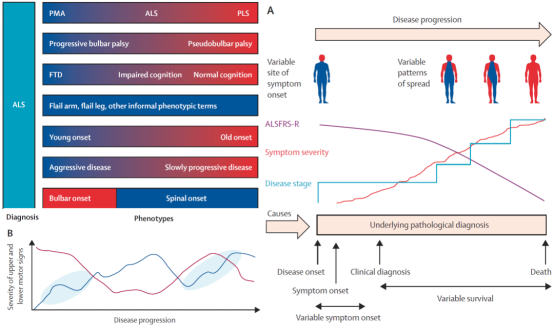
Notably, ALS is often accompanied by frontotemporal dementia. Patients without frontotemporal dementia, like Stephen Hawking, do not experience significant impairment in cognitive ability.
In many cases, there are also clear differences between early-onset and late-onset ALS. For example, a significant number of patients with early-onset disease survive beyond 10 years after diagnosis, and most late-onset patients have a very rapid course of disease, such as Stephen Hillenburg, the creator of SpongeBob SquarePants.
It is difficult to classify ALS because of its complex range of symptoms and pathological conditions, as well as the varying course of disease in different patients. Even among patients of the same age and with the same initial symptoms, the progression of disease and survival time vary widely. Therefore, it is very necessary and urgent to establish a clear ALS classification system. In addition to the UMN and LMN-based impairment types, ALS can also be subdivided into bulbar-onset ALS and spinal-onset ALS.
Treatments
Currently, there are only two drugs on the market for ALS:
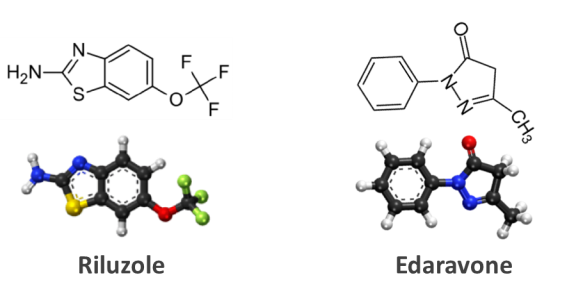
Other drugs can only relieve the complications faced by ALS patients, and their effects mainly include reducing neuralgia and fatigue, relaxing muscles, anti-spasticity, and suppressing external symptoms such as drooling and phlegm. In addition, there are some anti-depressants, antianxiety, and other psychotropic drugs, that are helpful for maintaining cognitive function.
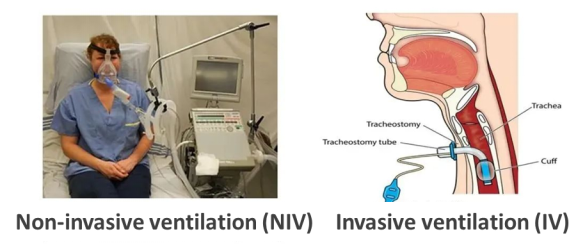
There are also assistant treatments that help relieve ALS symptoms:
RDDC Aids the Research of Rare Diseases
The Rare Diseases Data Center (RDDC) was developed by the Research Institute of Tsinghua, Pearl River Delta (RITPRD) with assistanbce from Cyagen Biosciences.
The RDDC database has collected and sorted out all information about rare diseases from international public biological resources, including related genes, mutations, phenotypes, and animal models of rare diseases, aiming to present them with added visualization capabilities. At present, the RDDC has collected information on over 20,000 genes and 14,000 human diseases!
Users are not only able to better understand the information of corresponding rare diseases, but also can take advantage of various AI tools to predict pathogenicity and RNA splicing patterns, so as to help speed up the research and development of treatments for rare diseases.
Click the photo above for more information!
*Statement: RDDC data and tools are only for scientific research reference, and should not be used as the final conclusion in medical diagnosis and evaluation.
[1] Dale Purves et al. Neuroscience.Sinauer Associates.2018.9781605353807,1605353809
[3] Al-Chalabi A , Hardiman O ,Kiernan M C , et al. Amyotrophic lateral sclerosis: moving towards a newclassification system[J]. Lancet Neurology, 2016, 15(11):1182-1194.
We will respond to you in 1-2 business days.